

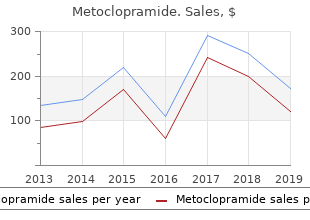
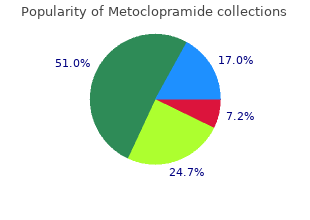
Metoclopramide
University Centre West Anglia at The College of West Anglia. I. Basir, MD: "Order online Metoclopramide no RX. Effective Metoclopramide OTC.".
Renal and serum cryoglobulin discount metoclopramide 10mg with mastercard gastritis black stool, they should be administered in involvement in essential mixed cryoglobulinemia purchase metoclopramide paypal gastritis or morning sickness. The latest attempt against the abnormal B-cell clones dri- Ann Intern Med 1992; 117: 573 buy metoclopramide in united states online gastritis diet rice. This agent has previously shown activity in B-cell populations in the blood and liver of patients with chronic lymphomas and autoimmune disorders buy metoclopramide with paypal gastritis diet 2013. Arthritis Rheum 2004; 50: showed rituximab resulted in a significant and rapid improve- 3668�78. Treatment of refractory, symptomatic, hepatitis C virus related mixed cryoglobulinemia with ribavirin and interferon-alpha. IgG and IgM cryoglobulins and fac- treatment of mixed cryoglobulinemia resistant to interferon a tors affecting cryoprecipitability. This is a relatively common condition characterized clinically by the development of palpable purpuric rash over the lower limbs, buttocks, and forearms. With the exception of the skin, other organs and tissues such as joints and kidneys may also be involved. The main symptoms and signs are palpable purpura, fever, arthralgia, proteinuria, and microscopic hematuria. Histological examination of purpuric lesions reveals prominent vasculitis with endothelial swelling, intense polymorph or lymphocyte infiltration, and disintegration of polymorphs (leucocytoclasis), resulting in ��nuclear dust��. The small blood vessels may also be thrombosed with fibrinoid changes and epidermal necrosis. Certain features, such as the prominent involvement blood vessel vasculitis which is believed to be secondary of the skin and the observation that these vasculitic syndromes to hypersensitivity mechanisms (1, 2, 3, 4). It may be the primary manifestation of a disease History and Classification (like in cutaneous leukocytoclastic angiitis) or, alternatively, a secondary component of another primary disease (like in A broad and heterogenous group of syndromes may result autoimmune diseases or malignancies). In many patients, been major impediments to the development of a coherent no inciting antigen could be found (7). Criterion Definition Age at disease onset Development of symptoms after age 16 >16 years Medication at disease Medication was taken at the onset of onset symptoms that may have been a precipitating factor Palpable purpura Slightly elevated purpuric rash over one or more areas of the skin; does not blanch with pressure and is not related to thrombocytopenia Maculopapular rash Flat and raised lesions of various sizes over one or more areas of the skin Biopsy including Histological changes showing granulocytes in arteriole and venule a perivascular extravascular location ahypersensitivity vasculitis is defined if at least 3 of these 5 criteria are present. The American College of Rheumatology 1990 criteria for the classification of hypersensitivity vasculitis. Immunopathogenesis Zeek, in his first classification scheme for vasculitides, coined the term ��hypersensitivity�� for allergic vasculitis in relation to animal models of vasculitis induced by the administration of exogenous antigens (allergens) such as horse serum and sulfonamides (8). In this animal vascu- litic model, a prominent cutaneous involvement has been observed together with involvement of small blood ves- sels, i. The identification of an inciting antigen in this model raised the possibility of an immune-complex mechanism. Thus, the and malignancies and also to related clinical entities 1994 Chapel Hill Consensus Conference on nomenclature such as serum sickness, urticarial vasculitis, and cuta- of the vasculitides (9) proposed an alternative term for neous vasculitis. A number of nonvasculitic diseases may also produce some or all of these abnormalities. Thus, the sometimes, to establish a more defined diagnosis (see clinical approach should especially exclude certain infec- Table 28. If an offending antigen, such as a drug, is tious diseases such as Rocky Mountain spotted fever, recognized, it should be removed if possible. If an under- Lyme disease, syphilis, disseminated gonococcal infec- lying disease such as an infection or a neoplasm is recog- tion, and some cases of bacterial endocarditis (most nized, it should be treated appropriately. If there is no cases of bacterial endocarditis produce small-vessel vas- recognizable underlying disease, treatment should be culitic disease). Also, atrial myxoma and cocaine abuse initiated according to the clinical manifestations that are should be considered and excluded. Immunofluores- established immunopathological studies, with the demon- cence staining shows variable quantities of immunoglo- stration of circulating IgA immune complexes and IgA bulin (mostly IgG) and complement deposition.
Many other terms are used to described different types of pelves but reference to them is not relevant here quality 10 mg metoclopramide gastritis ka desi ilaj. The diameters of the pelvic inlet and outlet as measured on the bony pelvis have been given in Chapter 9 order discount metoclopramide on line treating gastritis without drugs. They may occur through the superior or inferior ischiopubic ramus metoclopramide 10 mg with amex gastritis nutrition therapy, near the junction of the pubis and ischium (when they may involve the acetabulum) purchase metoclopramide with a mastercard gastritis daily diet, or the lateral part of the ilium. Isolated fractures of one part of the pelvis are usually not serious as long as the ring formed by the two hip bones and sacrum is not disrupted. When disruption occurs, there can be injury to the urinary bladder, the urethra, the rectum, or the vagina. In serious disruption of the pelvis, there may be permanent damage to nerves of the lumbosacral plexus. When a fracture of the pelvis involves the acetabulum, it can eventually lead to osteoarthritis at the hip joint. Extremely strong contraction of muscles (in competitive sports) can tear off a tendon from its attachment along with a small piece of bone. The cavity within the abdomen can be divided into a large upper part, the abdominal cavity proper; and a lower part, the pelvic cavity, which lies within the true pelvis (25. Superiorly, the abdominal cavity is bounded by the diaphragm, which separates it from the cavity of the thorax. We have seen that the domes of the diaphragm reach much above the level of the costal margin. As a result of this fact, a considerable part of the abdominal cavity lies deep to the thoracic cage. The abdominal organs lying in this part of the cavity are separated from pleurae and lungs only by the diaphragm. Note that the gluteal region lies behind the lower part of the abdominal cavity, and the pelvic cavity. The constitution of the anterior and posterior walls of the abdomen can be understood by examining a transverse section through the wall (25. Still more laterally, the posterior wall is formed by a muscle called the quadratus lumborum. The part of the abdominal wall extending all the way from the midline (in front) to the lateral edge of the quadratus lumborum is referred to as the anterior abdominal wall. However, note that it is not confned to the anterior aspect of the abdomen, but covers it from the lateral side as well. Next to the midline, the wall is formed by the rectus abdominis muscle that runs vertically. Between the lateral edge of the rectus abdominis and the lateral edge of the quadratus lumborum the anterolateral wall is made up of three layers of muscle. From outside to inside, these layers are formed by the external oblique, internal oblique and transverse muscles of the abdomen. These three are collectively referred to as the anterolateral muscles of the abdominal wall. The innermost layer of muscle is lined by a fascia called the fascia transversalis. The fascia transversalis is covered on the inside by parietal peritoneum, the two being separated by a layer of extraperitoneal fat. At the costal margin, the anterior abdominal wall becomes continuous with the thoracic wall. The external oblique muscle of the abdomen corresponds in position, and in the direction of its fbres, to the external intercostal muscle.
Peri- Male 0 portal hepatocytes may be organized forming rosettes Ratio of elevation of surrounded by lymphocytes and plasma cells generic 10mg metoclopramide gastritis red flags. Such infiltrate patients should receive treatment for each one of their None of the above A3 diseases buy 10 mg metoclopramide with visa prepyloric gastritis definition, steroids and ursodeoxycholic acid buy metoclopramide toronto gastritis y sintomas. Before the Treatment introduction of immunosuppressive therapy survival was reduced buy metoclopramide 10 mg gastritis cronica, particularly in jaundiced patients. Standard patients the prognosis is good, even in those with cirrhosis, treatment is either prednisone or prednisolone alone or a because most of them are good responders. In nonre- Prednisone monotherapy is preferred in children and young sponders patients, in those with suboptimal response and adults, while combination therapy is preferred in adult and in those with multiple relapses when treatment is with- old patients, in order to give lower doses of steroids, and in drawn, the prognosis is not so good, because they have a this way to minimize adverse effects of long-term treatment high probability to develop liver cirrhosis (12). The use of other immunosuppressive drugs � Reduction by 5 mg every 10 days or 10 mg every two weeks until should also be recommended in patients who developed normalization of transaminases � After remission is reached maintenance dose 10�15 mg/day severe adverse effects with steroids. Pregnant patients with compensated cirrhosis must � Cessation of therapyafter at least 2 yearsof remission, and doblood be submitted to an esophageal examination to assess the tests every 1 or 2 months for 6 months to detect relapse. Lancet schedule, but maintain a fixed dose of 50 mg/day of azathioprine 1956; 2: 1323�1326. The nature and prognostic implications of autoimmune hepatitis with acute presenta- tion. Chazouillieres O, Wendum D, Serfaty L, Montembault S, serum transaminase value (14). Primary biliary cirrhosis-autoim- a low-dose immunosuppressive treatment (5�10 mg of mune hepatitis overlap syndrome: clinical features and prednisone or 100 mg of azathioprine) should be continued response therapy. Diagnosis and treatment of autoim- for at least 2 years to reduce the risk of relapse. Autoimmune liver disease: overlap and not be withdrawn in any patient who has not achieved outliers. Autoimmune hepatitis, from mechan- with normal biochemistry for two years treatment can be ism to therapy. Am J patient experiences a relapse after withdrawal of immuno- Gastroenterol 2007; 102: 1013�1015. Am J not achieved with the combination of prednisone and Gastroenterol 2004; 99: 1510�1516. Current therapy for autoim- drug, such as tacrolimus, cyclosporin A or mycofenolate- mune hepatitis. Nature Clin Pract Gastroenterol Hepatol, mophetil, is recommended, since the risk of progression to 2007; 4: 202�214. Several animal models have been described, whereas multiple candidates have been proposed to initiate disease in a genetically susceptible host by molecular mimicry. The natural history of the disease may vary widely whereas no prognostic indexes are currently accepted. The only established medical treatment is based on ursodeoxycholic acid whereas liver transplantation is required in end stages. These cells are critical to the breakdown of tolerance by initiating the autoimmune response by T and B cells that ultimately mediate the onset of the liver injury. Signs and symptoms at presentation are illustrated in Four different stages are recognized according to Ludwig Table 55. Liver trans- plantation still represents the only effective treatment for the end stage of this disease with good survival rates. It is of note that the proposed definition of ��probable�� tory cases rifampicin can be used for a limited time.
The central processes of these neurons enter the spinal cord and terminate in relation to spinal grey matter buy discount metoclopramide online gastritis diet 2 days. They may ascend in the dorsolateral tract (situated near the tip of the dorsal grey column buy metoclopramide american express gastritis diet ayurveda, 50 buy metoclopramide online now gastritis pernicious anemia. The axons of these neurons constitute the anterior and lateral spinothalamic tracts discount 10 mg metoclopramide with mastercard gastritis nunca mas. The fbres for the lateral spinothalamic tract cross within the same segment of the cord, while those of the anterior spinothalamic tract may ascend for one or more segments before they cross to the opposite side. This tract merges with the medial lemniscus in the medulla and travels in the lemniscus to the thalamus. They ascend through the medulla, pons and midbrain (where this tract is often referred to as the spinal lemniscus) to end in the thalamus (ventral pos- terolateral nucleus). A number of tracts arising in spinal grey matter, and ending in masses of grey matter in the brainstem, are described. It carries impulses that regulate refex movements of the head and eyes in response to stimulation of some parts of the body. These pathways carry proprioceptive impulses arising in muscle spindles, Golgi tendon organs, and other receptors to the cerebellum. They constitute the afferent component of refex arcs involving the cerebellum for control of posture. The frst order neurons of these pathways are located in dorsal nerve root ganglia. Their peripheral processes end in relation to muscle spindles, Golgi tendon organs and other proprioceptive receptors. The central processes of the neurons concerned ascend in the posterior funiculi for varying distances before ending in spinal grey matter. Some of them ascend all the way to the medulla and end in the accessory cuneate nucleus. Neurons located in the dorsal nucleus (situated on the medial side of the base of the dorsal grey column in segments C8 to L3 of the spinal cord: 49. It ascends to the medulla where its fbres become incorporated in the inferior cerebellar peduncle and pass through it to reach the cerebellum (50. The fbres ascend in the lateral funic- ulus, anterior to the fbres of the dorsal spinocerebellar tract (50. At the upper end of the pons the fbres turn downwards to enter the superior cerebellar peduncle through which they reach the cerebellum (50. Interruption of ascending pathways carrying various sensations results in loss of sensory perception (anaes- thesia) over parts of the body concerned. In case of peripheral nerves the area of anaesthesia following injury is often much less than the area of distri- bution of the nerve. This is so because of considerable overlap in the areas supplied by different nerves. Dermatomes for adjoining seg- ments overlap, a given area of skin being innervated by two or more segments. In the case of spinal cord lesions, the level of disease can be inferred from the level of sensory loss. In this connection it must be remembered that the fner modalities of touch are carried by the posterior column tracts which are uncrossed. Crude touch, pain and temperature are carried by the spinothalamic tracts which are crossed. Thus, a unilateral lesion in the spinal cord can result in loss of the power of tactile localisation, tactile discrimination and of stereognosis on the side of lesion with loss of crude touch, pain and temperature on the opposite side.
Provocative testing is heartburn are suggestive of an esophageal source but based on the hypothesis that the esophagus is hyper- are often absent buy 10mg metoclopramide gastritis diet what to eat. Endoscopy is often used initially to exclude structural chest pain is simply an altered or heightened percep- or mucosal abnormalities such as erosive esophagitis buy 10 mg metoclopramide overnight delivery gastritis diet menus, tion of these stimuli cheap metoclopramide 10 mg without a prescription chronic antral gastritis definition. Most patients with noncardiac esophageal strictures/tumors purchase metoclopramide american express chronic gastritis outcome, achalasia, hiatal hernia, chest pain have personality traits similar to those of and gastric ulcers. This may or may not be manifested sion of a cholinergic agent (Tensilar), or in?ation of a by erosive esophagitis. Repro- result does not exclude re?ux, and re?ux may cause duction of cardiac-type pain is considered diagnostic of cardiac-type chest pain without symptoms of dysphagia an esophageal source of the pain. In addition, acid perfusion of the esopha- gus not only lowers the threshold for myocardial isch- emia but may induce this condition. Another commonly used �diagnos- of the Patient Care Committee of the American Gastrointestinal tic� test is a 2- to 4-week therapeutic trial with a proton Organization. Coronary ?ow reserve, esophageal motility, and chest pain in patients with angiographically dosage. Gastrointest then be prescribed, although the accuracy of this test Endosc Clin N Am 1994;4:731. An etiologic association noncardiac chest pain or dysphagia: results of three years� experience can be assumed if cardiac-type chest pain is temporally with 1161 patients. Motility disorders of the esophagus account for car- proton-pump inhibitors as a test for gastroesophageal re?ux disease: a diac-type chest pain in 5%�38% of patients evaluated meta-analysis of diagnostic test characteristics. Esophageal chest pain: current the pressure and function of the lower esophageal controversies in pathogenesis, diagnosis and therapy. Prevalence of esophageal Most motility abnormalities are intermittent and may disorders in patients with chest pain newly referred to the cardiologist. Belching, burping, and eructation have roughly the ?stula complicating a gastric carcinoma. In general, same meaning and refer to the passage of gas from the because gastric outlet obstruction or a carcinoma that stomach or esophagus through the mouth. In some is large enough to erode into the colon is likely to be patients, belching is the only symptom. However, in some patients with peptic dis- people swallow air in variable amounts, and all people ease who have a small ulcer or have erosions and gas- belch from time to time. This practice may be associated with psy- ally is made by ultrasonography of the upper abdomen. Perform a barium enema if the patient belches foul- lieve other abdominal symptoms. For unex- References plained reasons, patients who have symptomatic gall- American Gastroenterological Association website. How to help patients who to evaluate the stomach for partial gastric outlet ob- have troublesome abdominal gas. Dyspepsia is de?ned as chronic or recurrent pain or dyspepsia should be made cautiously to avoid unneces- discomfort centered in the upper abdomen, mainly in or sary cholecystectomy because gallstones may silently around the midline as opposed to the right or left hypo- coexist in patients with dyspepsia. Dyspepsia may or may not be related to eat- cause dyspepsia include potassium supplements, iron, ing meals.
Buy 10 mg metoclopramide with visa. NATURALLY CURE ACID REFLUX SAY GOOD BYE TO HEARTBURN.