

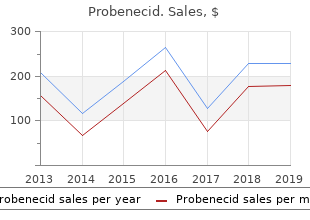
Probenecid
Hampshire College. E. Riordian, MD: "Purchase Probenecid. Cheap Probenecid OTC.".
Both forms of focal tachycardia inhibit normal sinus function symptoms ear infection, resulting in atrial tachycardia medications that cause constipation. Therapeutic management of focal (automatic) atrial tachycardia can usually be accomplished by transcatheter ablative techniques 4d medications. In the case of multiple symptoms of anemia, ectopic arrhyth- mogenic foci, surgeons have used more extensive and cre- ative ablative techniques, such as pulmonary vein isolation, left and right atrial isolation, and (for extreme cases) His bundle cryoablation coupled with pacemaker insertion. There effort to decrease cross clamp time, as the ablative procedure are two types of accessory connections: the manifest type, is performed before the reparative operation. This dissection exposes the entire left free-wall bypass tract is to divide or ablate the accessory connections that space to its boundaries, thereby ensuring division of any or all are responsible for the reentry phenomenon and clinical tachy- accessory connections. It requires Two surgical techniques, the endocardial and epicardial upward and rightward cardiac retraction for proper exposure, approaches, can be used. Cardiopulmonary bypass and aortic which frequently results in severe hemodynamic instability. Coronary sinus tributaries often require of a right free-wall connection, the dissection can be per- ligation and division, and care must be taken to avoid coronary formed without cardiopulmonary bypass. Results are excellent with either approach; the atrial end of all accessory connections in this area, except for choice generally depends on the preference and experience those immediately adjacent to the mitral valve annulus. Both the endocardial and epicardial techniques have Left free-wall ablation of an accessory connection is generally advantages and disadvantages; selection depends on the performed by the endocardial technique with cardiopulmo- anatomic circumstances associated with the operation. The surgeon should be familiar 2 mm, extending from the left fibrous trigone to the posterior with both techniques and be ready to alter the procedure septum (Fig. The endocar- dial technique approaches through the right atrium using car- diopulmonary bypass on a beating heart after all the precautions have been taken to ensure that there are no intracavitary shunts. The procedure is performed using a supra-annular incision 2 mm above the pos- terior medial tricuspid valve annulus, beginning at least 1 cm posterior to the His bundle. The supra-annular incision is extended counterclockwise onto the posterior right atrial free wall. The posterior septal space fat pad is then dissected away from the top of the posterior ventricular septum while the heart is beating, or during hypo- thermic cardioplegic arrest (Fig. The approach is dependent on the potential bleeding tendency that the dissec- tion plane creates and on the preference of the surgeon. Except for the location, the epicardial approach to poste- rior septal accessory connections is very similar to approach for left free-wall connections, as shown in Figure 18. The posterior septal accessory connections are interrupted by developing a dissection plane between the fat pad and the top of the posterior ventricular septum, following the mitral annulus over to the posterior superior process of the left ven- tricle, and following the epicardial reflection from the poste- rior right ventricle, across the crux, onto the posterior left ventricle. Cryoablation lesions are placed around the annulus to ensure complete division of all accessory connections. Except for location, this endocardial epicardium, establishing a dissection plane between the right dissection is similar to that for right free-wall lesions. Cryoablation lesions along the dissection clockwise direction onto the right anterior free wall. The dis- plane at the tricuspid annulus complete the accessory con- section plane is established between the fat pad occupying nection ablation. Under these circum- include unwanted entry into the right coronary artery and the stances, using cardioplegic arrest, a supra-annular incision is aortic wall at the right coronary sinus of Valsalva. The dissection is extended to the epicardial Patients with Ebstein’s anomaly of the tricuspid valve and reflection off the ventricle, thereby dividing all the penetrat- those with congenitally corrected transposition of the great ing fibers in this area. The incision can then be closed using arteries with Ebstein’s malformation of the systemic tricus- running suture technique.
Molecular weight 1058 ● Ciclosporin: increased fidaxomicin levels medications you can take while nursing, (daltons) avoid concomitant use treatment quadriceps tendonitis. Tirty-nine per cent of the dose whose creatinine clearance is as low as was excreted in the urine in the form of 9 mL/min treatment 5th metatarsal avulsion fracture. No studies have been done in metabolites (virtually no unchanged drug patients with creatinine clearance of less than was excreted in the urine) and 57% of total 9 mL/min medicine keeper. Volume of distribution 940–1460 litres ● Antifungals: concentration increased by (L/kg) ketoconazole. Flecainide is extensively metabolised ● Antimalarials: concentration increased (subject to genetic polymorphism), the two by quinine; avoid concomitant use with major metabolites being m-O-dealkylated artemether/lumefantrine. Haemodialysis increased by fosamprenavir, indinavir, removes only about 1% of unchanged lopinavir, ritonavir and saquinavir, flecainide. Pharmacokinetics nanograms/mL may be needed to obtain of newer drugs in patients with renal the maximum therapeutic effect. Fluconazole is metabolised only to a minor ● Antidiabetics: possibly enhances extent. Of a radioactive dose, only 11% is hypoglycaemic effect of nateglinide; excreted as metabolites in the urine. Fluconazole clearance is ● Antimalarials: avoid concomitant proportional to creatinine clearance. Antibiotic dosing in critically ill adult patients receiving continuous renal replacement therapy. A small ● Bone marrow suppression more common amount of flucytosine may be metabolised to in patients with renal impairment. Te pharmacokinetics of ● Approximately 60% of an administered fludarabine show considerable inter- dose is excreted in the urine within 24 hrs. Volume of distribution Widely distributed ● Antifungals: increased risk of (L/kg) hypokalaemia with amphotericin – Half-life – normal/ 3. In human ● Vaccines: high dose corticosteroids can volunteers, excretion through urine was impair immune response to vaccines – about 80%, and it was concluded that about avoid concomitant use with live vaccines. Elimination of radiolabelled drug is essentially complete within 72 hours, with 90–95% of the radioactivity appearing in urine and 5–10% in the faeces. Chronic dosing: ● Antimalarials: avoid concomitant use with 4–6 days/Increased artemether/lumefantrine and piperaquine with artenimol. Te rate ● Antivirals: concentration possibly of urinary excretion of flurbiprofen and increased by ritonavir; increased risk of its two major metabolites ([2-(2-fluoro- haematological toxicity with zidovudine. Te two major metabolites artemether/lumefantrine and piperaquine showed negligible pharmacological activity. Te other metabolites are not expected to be ● Antipsychotics: concentration of pharmacologically active. Excretion is mainly asenapine, haloperidol, clozapine and in the urine; about 2% of a dose is excreted as olanzapine increased; increased risk of unchanged drug. Folate metabolites are eliminated ● Doses up to 15 mg daily have been used in in the urine and folate in excess of body cases of malabsorption. Although not fully evaluated, there is no ● Manufacturer advises to avoid in severe evidence of fondaparinux metabolism and in renal impairment due to increased risk of particular no evidence for the formation of bleeding. Fondaparinux is excreted ● Clearance of fondaparinux increases by up to 64–77% by the kidney as unchanged to 20% during haemodialysis. Te primary route increased by etravirine, consider reducing of metabolism of amprenavir is via the dose of fosamprenavir; concentration cytochrome P450 3A4 enzyme. Te primary reduced by lopinavir and tipranavir, route of elimination of amprenavir is via effect on lopinavir unpredictable – avoid; hepatic metabolism with less than 1% concentration possibly reduced by excreted unchanged in the urine and no nevirapine. Metabolites ● Anxiolytics and hypnotics: increased risk account for approximately 14% of the of prolonged sedation and respiratory administered amprenavir dose in the urine, depression with midazolam – avoid with and approximately 75% in the faeces.
In two cases treatment 1st degree heart block, a pedestrian was injured medicine x boston, five cases caused minor injury to a passenger not necessitating hospital admission symptoms 4 dpo, and in three cases medicine for nausea, a passenger incurred severe injuries. In only one case did the collision result in the death of others (two people in a shop). Deaths Caused by Motor Vehicle Accidents 281 Categories of Motor Vehicle Accidents Motor vehicle accidents can be divided into four categories, depending on how the accident occurred: 1. Rear impact crashes The probability of a fatality depends to a degree on the size and type of vehicle involved in a crash. Utility vehicles and pickups are generally heavier than are automobiles, therefore, the occupants of the former vehicles are more likely to survive crashes with cars. Pickups and sports utility vehicles, however, are more likely than cars to be involved in fatal single-vehicle crashes. Deaths are slightly more common in multiple vehicle crashes than single vehicle crashes. In fatal single vehicle crashes involving a car, the frequency of the type of crash causing death, in descending order, is: frontal impact; side impact, rollover and rear impact. In fatal multi- vehicle crashes involving a car, the frequency of type of crash in descending order is: frontal and side impacts (approximately equal), followed by rear impacts and then rollovers. For pickups and utility vehicles, it is frontal impact; side impact; rear impact and finally rollover. Front Impact Crashes Front impact crashes are the type of crash that most people think of when talking about motor vehicle accidents. Textbooks tend to concentrate on this type of accident, because it is easy to explain and understand. When two vehicles crash head-on, or a vehicle crashes into a fixed object, unless the driver and passengers are restrained, they will continue their forward move- ment, even though the car has stopped. If unrestrained, the driver’s knees will impact the instrument panel; the chest the steering wheel; and the head the windshield, sun visor region above the windshield, or the frame (generally in this order). The same pattern of injuries would be true for unrestrained passengers, except they would impact the dashboard rather than the steering wheel. If the front impact is off-center, the driver or passenger might impact the A pillar with their head. Unrestrained individuals in the back seat will hit the back of the front seat, the passengers in the front seat come up against the windshield or the sun visor area. Objects protruding from the instrument panel, such as levers or knobs, can produce patterned abrasions on the victims. If the drivers and passengers have restraint devices and if the passen- ger compartment retains its integrity, then the occupants of the vehicle should survive without any significant injury. The intrusion of part of the vehicle or another object into the passenger compartment may be transitory, with the portion of car or the object springing back. Thus, it might not at first be obvious that there has been violation of the integrity of the passenger compartment. If the head of the driver or front seat passenger impacts the windshield, there will be abrasions and superficial cuts of the forehead, nose, and face, with the injuries having a vertical orientation (Figure 9. The glass cuts, per se, are not serious, thanks to the construction of the windshield.
The minimum acceptable graft-to-body weight ratio to provide adequate postop liver function is 1% medications januvia. However medicine hat lodge, the suitability of a donor is more often determined by the maximum amount of donor liver that a recipient can accommodate in the abdominal cavity medicine to reduce swelling. This results in the utilization of several different types of grafts in pediatric liver transplantation pretreatment. Although the type of graft used determines certain technical aspects of the hepatectomy and implantation, the general sequence of events consists of: 1. Anhepatic phase (during which portal venous inflow and hepatic venous outflow are reconstituted) 3. Biliary reconstruction A bilateral subcostal incision is used with a midline subxiphoid extension as needed. The abdomen is explored, and adhesions are lysed taking care to suture- ligate varices in patients with portal hypertension. This portion of the procedure may be tedious and bloody in patients with prior liver surgery. The left coronary ligament is divided, and the left lateral segment is mobilized from the diaphragm. The peritoneum of the hepatoduodenal ligament is divided, and a hilar dissection is performed. The connective and vascular tissue of the hepatoduodenal ligament is carefully divided taking care to suture-ligate any varices en masse until the common bile duct is identified. This portion of the procedure may result in significant blood loss in patients with severe portal hypertension and coagulopathy. The common bile duct is then suture-ligated and divided high in the hilum of the liver. The right lobe of the liver is mobilized from its retroperitoneal attachments to expose the lateral border of the vena cava. In the standard technique the infra and suprahepatic vena cava are encircled taking care not to injure the right adrenal vein, right renal vein, or inferior phrenic veins. The portal inflow is occluded with a vascular clamp followed by occlusion of the infrahepatic and suprahepatic vena cava. At this point, the patient must have adequate circulatory volume to support the interruption of subdiaphragmatic venous return to the heart without developing vasopressor refractory hypotension. Although this degree of circulatory compromise is typically well tolerated by very young children and those with chronic portal hypertension, venous congestion can result in troublesome intestinal edema and hemodynamic compromise in metabolic patients or those with fulminant hepatic failure who lack alternative variceal pathways of venous return. The recipient liver and retrohepatic vena cava are excised, and donor liver implantation begins. In the piggyback technique, which is used in the living donor operation, the liver is completely mobilized from the retrohepatic vena cava by individually ligating the short hepatic veins draining directly from the liver to the cava. The liver is excised with preservation of the retrohepatic vena cava, and venous return can be restored prior to implantation by moving the vascular clamp to the junction of the vena cava with the hepatic veins. The goal of the surgical team during the anhepatic phase is to minimize the duration of caval disruption with its associated intestinal edema and variceal congestion. The hepatic vein outflow is first reconstructed by fashioning the suprahepatic caval anastomosis. In the piggyback technique, there is no infrahepatic caval anastomosis and an end-to-end portal vein anastomosis is fashioned next. The liver is flushed + with Custodiol solution (low K , buffered donor organ transplant solution) or + albumin prior to reperfusion to minimize the risk of cardiac arrest 2° ↑ K and ↓ pH.
The presence of degenerative arthritic changes medications ranitidine, loss of disc height symptoms 2 months pregnant, bulging discs medications54583, and ligamentum flavum can dis- tort and limit the space significantly symptoms 13dpo. Reported complica- tions followed the growing use of epidural steroid injections at the C5 level. Epidural abscess formation is usually 10–15 days later and may present with fever or worsened neurologic com- plaints. Dural puncture or tear with or without postdural When satisfactory needle position is confirmed, a contrast- puncture headache is another complication, which is more filled T-piece is carefully connected to the epidural needle. Hydration The use of the T-piece allows for aspiration and injection and bed rest are first-line treatments. The syringe containing patch are two treatments for refractory postdural puncture the drugs to be injected is attached to the T-piece. Rarely, patients with postdural puncture head- ache develop intracranial subdural hematomas. Other rare vertent dural puncture can occur in the best of hands, and careful observation for spinal fluid is mandatory. Possible complications are adjusted accordingly because subarachnoid migration of summarized in Table 8-1. If no blood is present, incremental taneous tissues, the styleted epidural needle impinges on doses of local anesthetic and other drugs may be adminis- the ligamentum nuchae, which runs vertically between the tered while the patient is monitored closely for signs of apices of the cervical spinous processes. Pain, numbness, or other worrisome symptom dur- This ligament is dense enough to hold a needle in position ing injection may signal neural compression, and it might even when the needle is released. The interspinous ligament, which runs obliquely between the spinous processes, is encountered next and offers additional resistance to needle advancement. This steroid injections may be due to different criteria for study phenomenon is more pronounced in the cervical region inclusion in each meta-analysis. The applicability to cervical than in the lumbar region because the ligaments are less spine syndromes is unknown; however, several recent studies well defined. Buttermann reported a randomized trial of A significant increase in resistance to needle advance- lumbar epidural steroid injections versus surgical discectomy ment signals that the needle tip is impinging on the dense and found epidural steroid injections to have benefit. Because the ligament is made up al- tients had similar pain scores in the long term but a signifi- most entirely of elastin fibers, resistance increases as the cant number of patients crossed over from the injection needle traverses the ligamentum flavum because of the 27 group to surgery. There should but did not change the surgery rate in patients with disk be essentially no resistance to injecting the drug into the herniations. On the 12- Epidural hematoma month follow-up, following the lysis procedure for spinal Cardiopulmonary arrest stenosis, epidural steroid injection followed by hypertonic Bowel or bladder loss of function saline was significantly effective. Also, some patients will unavoidably choose surgery due to Spinal Neuroaxial Procedures 135 inadequate pain relief. The use of epidural injections for likely to have anterior segmental arteries supplying the other diagnoses is common, but fewer data are available re- anterior spinal artery. Be- ■ Inability to lie in prone or in lateral decubitus cause of the narrowness and potential for profound spinal position cord injury, fluoroscopy was introduced as a safety tool for ■ Significant central spinal stenosis the pain physician. Naturally, the use of nonionic, water- ■ Syrinx soluble radiographic contrast was soon added to monitor vascular runoff. Cl and C2 nerve roots exit the central neuraxis ■ Two 10-ml syringes posteriorly through the intralaminar space to innervate the ■ Needle holder posterior upper neck and scalp of the occipital region.
. Afrikaans Primary HIV Symptoms (Simptome van Primêre MIV Infeksie).