

Fosamax
College of Saint Benedict. X. Jack, MD: "Order cheap Fosamax no RX. Proven Fosamax online.".
The schistosomulae migrate through several tissues and stages to their residence in the veins order fosamax online pills women's health center victoria tx. Courtesy of Centers for Disease occurs when schistosomes infect the liver Control and Prevention/Edwin P best buy fosamax pregnancy pillow. Histopathology of the bladder shows eggs of S haematobium surrounded by intense infltrates of eosinophils purchase 35 mg fosamax with mastercard menstrual molimina. Clinical Manifestations Epidemiology Shigella species primarily infect the large Humans are the natural host for Shigella intestine discount fosamax 35mg on-line women's health nurse practitioner salary by state, causing clinical manifestations that organisms, although other primates can be range from watery or loose stools with mini- infected. The primary mode of transmission mal or no constitutional symptoms to more is fecal-oral, although transmission can also severe symptoms, including high fever, abdom- occur via contact with a contaminated inani- inal cramps or tenderness, tenesmus, and mate object, ingestion of contaminated food mucoid stools with or without blood. Housefies may dysenteriae serotype 1 ofen causes a more also be vectors through physical transport of severe illness than other shigellae with a higher infected feces. Ingestion of as few as 10 organ- risk of complications, including septicemia, isms, depending on the species, is sufcient pseudomembranous colitis, toxic megacolon, for infection to occur. Prolonged organism intestinal perforation, hemolysis, and hemo- survival in water (up to 6 months) and food lytic uremic syndrome. Chil- to S dysenteriae 1 has become rare in industri- dren 5 years or younger in child care settings alized countries. Generalized seizures have and their caregivers, people living in crowded been reported among young children with conditions, and men who have sex with men shigellosis attributable to any serotype; are at increased risk of infection. Infections although the pathophysiology and incidence attributable to S fexneri, S boydii, and are poorly understood, such seizures are S dysenteriae are more common in older chil- usually self-limited and associated with high dren and adults than are infections attributable fever or electrolyte abnormalities. Septicemia to S sonnei in the United States; nonetheless, is rare during the course of illness and is more than 25% of cases caused by each species caused by Shigella organisms or by other are reported among children younger than gut fora that gain access to the bloodstream 5 years. Travel to resource-limited countries through intestinal mucosa damaged during with inadequate sanitation can place travelers shigellosis. Even without antimicrobial neonates, malnourished children, and people therapy, the carrier state usually ceases within with S dysenteriae 1 infection. Reactive arthri- 1 to 4 weeks afer onset of illness; long-term this with possible extraarticular manifestations carriage is uncommon and does not correlate is a rare complication that can develop weeks with underlying intestinal dysfunction. Shigella species are facultative aerobic, gram- Diagnostic Tests negative bacilli in the family Enterobacteriaceae. Isolation of Shigella organisms from feces or Four species (with more than 40 serotypes) rectal swab specimens containing feces is have been identifed. Among Shigella isolates diagnostic; sensitivity is improved by testing reported in the United States in 2012, approx- stool as soon as possible afer it is passed. The imately 81% were Shigella sonnei, 17% were presence of fecal lactoferrin (or fecal leuko- Shigella fexneri, 1% was Shigella boydii, and cytes) demonstrated on a methylene-blue� less than 1% was other species. In resource- stained stool smear is fairly sensitive for the limited countries, especially in Africa and diagnosis of colitis but is not specifc for Asia, S fexneri predominates, and S dysenteriae shigellosis. Shiga toxin is produced blood should be cultured in children who by S dysenteriae 1, which enhances virulence at are severely ill, immunocompromised, or malnourished. Treatment For cases in which treatment is required and susceptibilities are unknown or an Although severe dehydration is rare with ampicillin- and trimethoprim-sulfamethoxazole� shigellosis, correction of fuid and electrolyte resistant strain is isolated, parenteral cefriax- losses, preferably by oral rehydration solutions, one for 2 to 5 days, a fuoroquinolone (eg, is the mainstay of treatment. Most clinical ciprofoxacin) for 3 days, or azithromycin for infections with S sonnei are self-limited (48� 3 days should be administered.
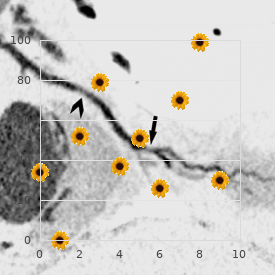
Multiple antigenic types cocirculate tion of viral antigen in stool or antibody in in the same region purchase cheap fosamax on line menstruation nation. Of these young children in the community but appear tests discount 70 mg fosamax visa menstrual uncleanness, reverse transcriptase-polymerase chain to cause a lower proportion of cases of more reaction assay is the most sensitive cheap fosamax 35 mg visa menstruation urinalysis. Astrovirus infec- Treatment tions occur predominantly in children younger No specifc antiviral therapy is available order genuine fosamax on-line menopause 35 years old. Oral than 4 years and have a seasonal peak during or parenteral fuids and electrolytes are given the late winter and spring in the United States. Panel A: special staining identifes astrovirus in the brain of the patient; Panel B: histopathological changes in brain tissue. Although more than 100 pathogens have been identifed as causative agents, the pathogen is not determined for up to 75% of cases. This diagnostic failure impedes effective treatment and underscores the need for better tools and new approaches for detecting novel pathogens or determining new manifestations of known pathogens. Although astroviruses are commonly associated with gastroenteritis, they have not been associated with central nervous system disease. Humans become The infection also can be severe and life threat- infected through tick bites, which typically are ening, particularly in people who are asplenic, not noticed. Babesiosis, virginianus) is an important host for blood like malaria, is characterized by the presence meals for the tick but is not a reservoir host of of fever and hemolytic anemia; however, some B microti. An increase in the deer population infected people who are immunocompromised in some geographic areas, including some sub- or at the extremes of age (eg, preterm new- urban areas, during the past few decades is borns) are afebrile. Tere can be a prodromal thought to be a major factor in the spread of illness, with gradual onset of symptoms, such I scapularis and the increase in numbers of as malaise, anorexia, and fatigue, followed by reported cases of babesiosis. The reported development of fever and other infuenzalike vector-borne cases of B microti infection have symptoms (eg, chills, sweats, myalgia, arthral- been acquired in the Northeast (particularly, gia, headache, anorexia, nausea). Less common but not exclusively, in Connecticut, Massachu- features include sore throat, nonproductive setts, New Jersey, New York, and Rhode Island) cough, abdominal pain, vomiting, weight loss, and in the upper Midwest (Wisconsin and conjunctival injection, photophobia, emotional Minnesota). Congenital infec- siosis caused by other species have been tion with manifestation as severe sepsis syn- described in various regions of the United drome has been reported. States; tick vectors and reservoir hosts for these Clinical signs generally are minimal, ofen agents typically have not yet been identifed. If untreated, illness can last for several weeks 1 to 5 weeks afer a tick bite; 1 week afer a con- or months; even asymptomatic people can have taminated blood transfusion but occasionally persistent low-level parasitemia, sometimes for is longer (eg, latent infection might become longer than 1 year. Acute, symptomatic cases of babesiosis are typ- The etiologic agents of babesiosis in the United ically diagnosed by microscopic identifcation States include Babesia microti, which is the of the organism on Giemsa- or Wright-stained cause of most reported cases, and several other blood smears. B microti and Epidemiology other Babesia species can be difcult to distin- Babesiosis predominantly is a tick-borne guish from Plasmodium falciparum; examina- zoonosis. Babesia parasites can also be trans- tion of blood smears by a reference laboratory mitted by blood transfusion and through peri- should be considered for confrmation of the natal routes. If indicated, the plus azithromycin is associated with fewer possibility of concurrent B burgdorferi or adverse efects. Exchange blood transfusions should be con- Treatment sidered for patients who are critically ill Clindamycin plus oral quinine for 7 to 10 days, (eg, hemodynamically unstable), especially, or atovaquone plus azithromycin for 7 to but not exclusively, for patients with parasit- 10 days, have comparable efcacy for mild to emia levels of 10% or more. A, the tetrad (left side of the image), a dividing form, is pathognomonic for Babesia.
Axial T1-weighted (A) and axial postgadolinium T1-weighted (B) images showing an enlarged liver with extensive metastatic disease from a primary cervical cancer order fosamax us menstrual bloating treatment. C: Coronal fat-suppressed T2-weighted image in the same patient showing right hydronephrosis secondary to ureteral obstruction by the primary malignancy discount fosamax 70mg with amex pregnancy 1st trimester. Coronal T2-weighted (A) and axial fat-suppressed postgadolinium T1-weighted (B) image showing a small pseudocyst (arrow) of the pancreatic head in a patient with acute pancreatitis buy cheap fosamax on line menopause pain. C: Axial T2-weighted view showing communication of the pseudocyst with a prominent pancreatic duct 70mg fosamax with mastercard womens health yakima wa. Coronal T2-weighted (D) and axial T2-weighted (E) images from a second patient showing a large hemorrhagic pseudocyst with very little normal residual tissue. A: Axial fat-suppressed postgadolinium T1-weighted image of pancreatic cancer of the head of the pancreas. B: Axial T2- weighted image showing the pancreatic cancer as well as dilation of the pancreatic duct. A: Coronal T2-weighted image thatshows a normal appendix (white arrow) and a gravid uterus (black arrow). B: Coronal T2-weighted image with an in?amed appendix (white arrow) and gravid uterus (black arrow). Mohan 4 progressing to widespread ?brosis of other organs, which may Indications be fatal. It is also helpful to indicate pertinent labora- a signi?cant change in the patient�s subsequent management tory work the patient has had prior to imaging and whether (9�18). The radiologist must be soft tissue edema or bone marrow edema and can elegantly informed about any potential renal compromise prior to demonstrate abscesses, interfascial ?uid collections, skin booking any cross-sectional imaging study. Iodinated radio- defects, and bony destruction, particularly when intravenous graphic contrast agents are usually not given if renal function gadolinium is given. Gradient echo sequences are also sensi- is compromised, particularly when associated with diabetes tive for picking up small bubbles of gas or metallic foreign mellitus, as these patients are at increased risk of developing bodies, manifesting as blooming areas of low-signal intensity contrast-induced nephropathy (1�3). Therefore, it is impor- 30 mL/minute, as this has been linked to the development of tant to correlate imaging ?ndings with the clinical nephrogenic systemic ?brosis, also known as nephrogenic presentation and to have some knowledge of the normal ?brosing dermopathy. This entity was ?rst described in 1997 anatomy of the musculoskeletal structures in the extremities and is characterized by skin thickening with inhibition of to avoid over-diagnosing pathology. Mohan Diagnostic capabilities demonstrate subtle pathology that may currently be over- looked with other imaging modalities. Fractures and dislocations are common and are almost always associated with injuries to intra-articular struc- Imaging pitfalls and limitations tures and surrounding soft tissues. However, children extent of associated soft tissue damage is often underesti- under the age of 6 years may ?nd it di?cult to remain still mated. Soft tissue swelling, joint e?usions, and joint space for the duration of the scan, thereby resulting in motion asymmetry are signs for increased clinical suspicion for asso- artifact. However, musculoskeletal 400 pounds and a maximum bore diameter of 70 cm, thereby ultrasound is very operator-dependent, and it can take con- excluding morbidly obese patients. The majority of radiology departments susceptibility artifact is created by metallic implants, particu- develop their own standard imaging protocols to ensure that larly those containing stainless steel (23). There are also a number of recently for demonstrating ?ne anatomic detail, and fat-saturated developed metal suppression sequences that can optimize ima- ?uid sensitive sequences such as T2 and proton density can ging around metal implants (24). Patients are usually imaged with the arm at the side, either at neutral or externally rotated for optimal visualization of rotator cu? tendons. Severe degenerative change of the acromioclavicular joint is evident (arrowhead), with lateral 587 down sloping of the acromion (open arrow), likely impinging on the supraspinatus tendon. There is subtle edema within the infraspinatus muscle (open arrows), indicative of early denervation. Grashey (A) and axillary (B) views of the left shoulder taken after a skiing injury show faint sclerosis (arrows) projecting over the margins of the greater tuberosity � but no obvious fracture line.
Syndromes
- HLA tissue typing (to find matching bone-marrow donors)
- Massage
- Liquid diet at first
- Excessive bleeding
- Nutcracker esophagus
- Pelvic laparoscopy
- Stroke
- You have had surgery on your carotid artery
- Coughing up blood
To avoid confusion cheap fosamax 35 mg with amex womens health diet pill, it is better to refer to ulcers in the stomach as gastric ulcers best 35 mg fosamax menstrual zits. From a functional point of view the mucosa of the stomach can be divided into an acid secreting proximal part (consisting of the fundus and greater part of the body); and a distal area (pyloric antrum and pyloric canal) the secretions of which are rich in mucous and are mildly alkaline cheap fosamax 35mg without prescription menopause 6 years after hysterectomy. The distal region also secretes gastrin which stimulates acid secretion by the proximal part cheap fosamax 70 mg online womens health 1500 calorie meal plan. The normal gastric mucosa is resistant to the action of acid present in the stomach. However, in some cases, the mucosa gets eroded leading to the formation of a gastric ulcer. Such ulcers are usually formed in the distal (alkaline secretion producing) area, near the lesser curvature. As the ulcer erodes further into the thickness of the stomach wall, it can result in adhesion of the stomach wall to surrounding structures, or to perforation of the wall. Perforation of an ulcer located on the posterior wall of the stomach can lead to leakage of contents into the lesser sac. It can also lead to erosion of the pancreas, and even of the splenic artery (the latter leading to fatal haem- orrhage). Perforation of an ulcer on the anterior wall of the stomach can lead to escape of gastric contents into the greater sac. In some cases, a partial gastrectomy (removing the distal gastrin producing part) can cure an ulcer. The lower end of the oesophagus and the frst part of the duodenum are also removed. Continuity of the gut is established by anastomosing the oesophagus with the jejunum. In cases of suspected gastric ulcer or carcinoma, the interior of the stomach can be viewed through a gastroscope. Radiologically, the gastric mucosa can be studied by taking skiagrams after a barium meal. It is in the form of a roughly C-shaped loop which is retroperitoneal and, therefore, fxed to the posterior abdominal wall. At its caudal end, the duodenum becomes continuous with the jejunum at the duodenojejunal flexure. The first or superior part begins at the pylorus and passes backwards, upwards and to the right. It passes from right to left (with a slight downward convexity) and crosses the midline at the level of the third lumbar vertebra. It runs upwards and to the left and ends by joining the jejunum at the duodenojejunal fexure. The junction of the superior and descending parts of the duodenum is called the superior duodenal flexure; while that between the descending and horizontal part is called the inferior duodenal flexure. S: Superior part; D: Descending part; H: Horizontal part; A: Ascending part 542 Part 4 � Abdom en and Pelvis want to know more? Covered by transverse mesocolon, and sometimes by transverse colon, and/or loops of jejunum. Chapter 27 � Oesophagus, Stom ach and Intestines 543 Ascending (Fourth) Part Anteriorly a.
Discount fosamax 35 mg online. Lynn Beauchamp MD | Women's Health | Mosaic Life Care.